
Four examples of outpatient medical decision making based visits
Let’s talk about “Medical Decision Making,” or MDM, for short. MDM is how you prove, in writing, that the cognitive work you did in the exam room (think building a differential diagnosis, documenting the visit, implementing a plan of care) was worth a certain dollar amount. Since 2021, the AMA has made MDM the preferred path to justifying your E&M level, meaning no more counting bullets in your HPI or obsessing over the review of systems. What matters now is how complex your thinking was.
MDM has three components: the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of the management plan. You need to meet a certain threshold on at least two of the three categories to hit a given level.
The stakes are real. A moderate established visit (i.e., 99214) pays roughly $50–$80 more than a low established visit (i.e., 99213) depending on your institutional policy. Let’s look at four practical scenarios and break down exactly why each one codes the way it does.
The four cases
Case 1 — the routine refill
You see an established patient with gastroesophageal reflux disease (GERD), which is stable at this time.
Plan: Continue current dose of omeprazole, 20 mg, once daily. Refills sent to pharmacy. Return in 12 months for follow-up, unless otherwise needed.

This is the bread-and-butter routine follow-up visit. Stable problem, no data reviewed, prescription continued without change. It hits low on problems (one stable chronic illness), minimal on data reviewed, and moderate on risk (prescription drug management). When categories are split like this, best to choose the average of the three, which in this case would be low.
Case 2 — the exacerbation
You see an established patient with gastroesophageal reflux disease (GERD), which has been worsening because of increased stress and anxiety at work.
Plan: Increase omeprazole from once daily to twice daily. Return to clinic in 3 months, or sooner if needed.

Same disease, different day. The patient’s condition is no longer stable. It’s been getting worse, which moves the problem complexity from low to moderate. Combine that with prescription management (moderate risk) and you meet the two-of-three bar at moderate. This is a 99214. The chart should say “exacerbation” or “worsening” to cue your billers to code, as such.
Case 3 - the new patient
You see a new patient, who presents with heartburn. His general practitioner (GP) started omeprazole for presumed reflux, with no improvement. You review the GP’s note during the visit.
Plan: Increase omeprazole to twice daily. Order CBC, BMP, and abdominal x-ray. Return to the clinic in 1 month for re-assessment.
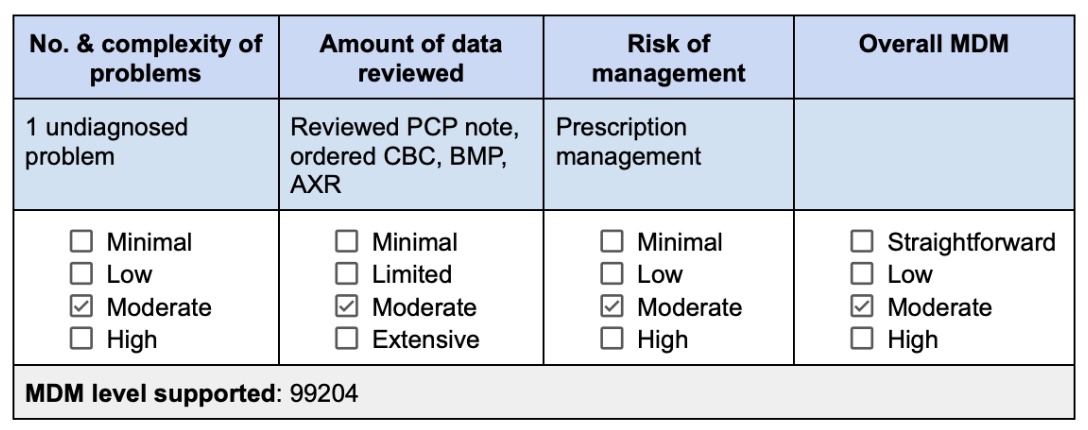
Here, all 3 categories meet criteria for moderate. You reviewed an external note (that’s one data point) and ordered three tests (that counts toward the data element, as well, because it is assumed that you will review them once resulted). An undiagnosed problem is also considered moderate. With all three categories meeting moderate, this is a clean 99204 for a new patient. Don’t forget to explicitly document that you reviewed the outside note, e.g., “Reviewed PCP note from [date].”
Case 4 — the procedure visit
You see a new patient with longstanding reflux. She reports persistent heartburn despite being on pantoprazole for the past 12 months. She also reports intermittent dysphagia. Her symptoms are exacerbated during times of stress and with certain meals
Plan: Esophagogastroduodenoscopy (EGD) with possible pH testing.
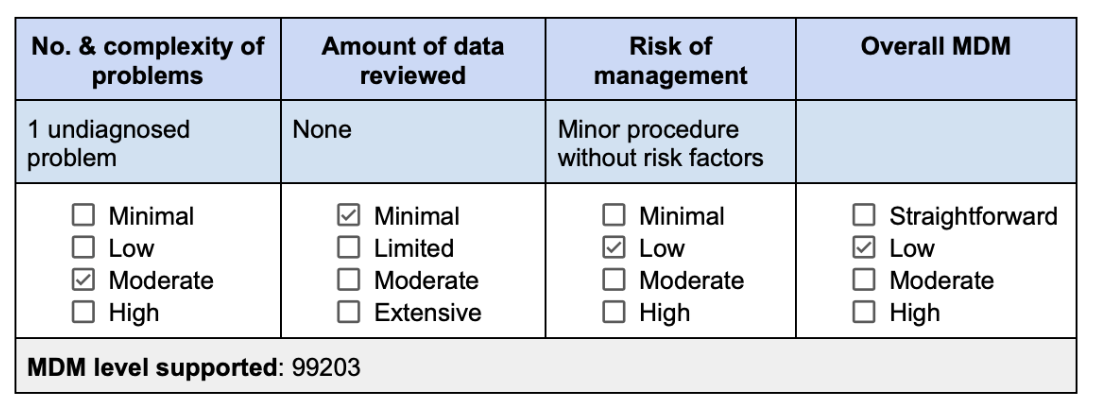
This visit sounds complex, right? But look at the grid. No data was reviewed at this visit. And the risk element hinges not on the diagnosis, but on the management plan. EGD is a minor procedure without identified risk factors — that puts risk at low. Splitting the difference between moderate and minimal makes this a low visit (99203) for a new patient.
The takeaways
Remember, the MDM table is not a formality but the receipt. “Undiagnosed problem,” “chronic illness with exacerbation,” “reviewed outside records” are requirements for reimbursement.
The physicians who master MDM don’t see more patients, don’t work longer hours, and don’t compromise clinical care. They just document what they already do. That’s the entire game.